
Concussion management in sports first aid
Concussion must be taken extremely seriously. If you suspect a player is suffering from concussion they must be removed from play immediately and assessed by a medical practitioner. Erring on the side of caution is important!
The definition of sport related concussion from the 2017 Concussion in Sport Group (CISG) following the 2016 international conference in Berlin is:
Sport related oncussion is a traumatic brain injury induced by biomechanical forces. Several common features that may be utilised in clinically defining the nature of a concussive head injury include:
- SRC may be caused either by a direct blow to the head, face, neck or elsewhere on the body with an ‘impulsive’ force transmitted to the head.
- SRC typically results in the rapid onset of short-lived impairment of neurological function that resolves spontaneously. However, in some cases, symptoms and signs evolve over a number of minutes to hours.
- SRC may result in neuropathological changes, but the acute clinical symptoms largely reflect a functional disturbance rather than a structural injury and, as such, no abnormality is seen on standard structural neuroimaging studies.
- SRC results in a range of clinical symptoms that may or may not involve loss of consciousness. Resolution of the clinical and cognitive features typically follows a sequential course. However, in some cases symptoms may be prolonged.
The clinical signs and symptoms cannot be explained by drug, alcohol, or medication use, other injuries (such as cervical injuries, peripheral vestibular dysfunction, etc) or other comorbidities (eg, psychological factors or coexisting medical conditions)
[ref: Consensus statement on concussion in sport, Berlin 2016]
In summary:
Sport related concussion is a complex process caused by trauma that transmits force to the brain either directly or indirectly and results in temporary impairment of brain function. Its development and resolution are rapid and spontaneous. A Player can sustain a concussion without losing consciousness. Concussion is associated with a range of clinical signs and symptoms that resolve sequentially. Concussion reflects a functional rather than structural injury and standard neuro-imaging is typically normal.
Sport Related Concussion Resources
From our downloads page you can find:
- SCAT5 Sport Concussion Assessment Tool version 5, April 2017
- Child SCAT5 Sport Concussion Assessment Tool for children ages 5 - 12 years version 5, April 20
- CRT5 Concussion Recognition Tool version 5, April 2017
- Consensus Statement on Concussion in Sport - 5th International Conference, Berlin 2016
How to recognise sport related concussion
- Symptoms: somatic (eg, headache), cognitive (eg, feeling like in a fog) and/or emotional symptoms (eg, lability)
- Physical signs (eg, loss of consciousness, amnesia, neurolog- ical deficit)
- Balance impairment (eg, gait unsteadiness)
- Behavioural changes (eg, irritability)
- Cognitive impairment (eg, slowed reaction times)
- Sleep/wake disturbance (eg, somnolence, drowsiness)
If signs or symptoms in any one or more of these domains are present then an SRC should be suspected.
Remember that a player doesn't have to be knocked out (lose consciousness) to experience a concussion. As a first aider you will be called upon to do and on-pitch or sideline evaluations of a player who has been involved in an incident with concussion producing forces. If you suspect that a player has concussion the player must be removed from the field of play and must not play any further part in the game. Continuing to play after sustaining a concussion may result in a more serious brain injury or a prolonged recovery period.
Treatment of sport related concussion
When a player shows any symptoms or signs of an SRC:
- The player should be evaluated by a physician or other li- censed healthcare provider on site using standard emergen- cy management principles, and particular attention should be given to excluding a cervical spine injury.
- The appropriate disposition of the player must be deter- mined by the treating healthcare provider in a timely man- ner. If no healthcare provider is available, the player should be safely removed from practice or play and urgent referral to a physician arranged.
- Once the first aid issues are addressed, an assessment of the concussive injury should be made using the SCAT5 or other sideline assessment tools.
- The player should not be left alone after the injury, and se- rial monitoring for deterioration is essential over the initial few hours after injury.
- A player with diagnosed SRC should not be allowed to return to play on the day of injury.
A key concept in sideline assessment is the rapid screening for a suspected SRC, rather than the definitive diagnosis of head injury.
Any athlete with a suspected concussion should be IMMEDIATELY REMOVED FROM PLAY, and should not be returned to activity until they are assessed medically. Athletes with a suspected concussion should not be left alone and should not drive a motor vehicle.
It is recommended that, in all cases of suspected concussion, the player is referred to a medical professional for diagnosis and guidance as well as return to play decisions, even if the symptoms resolve.
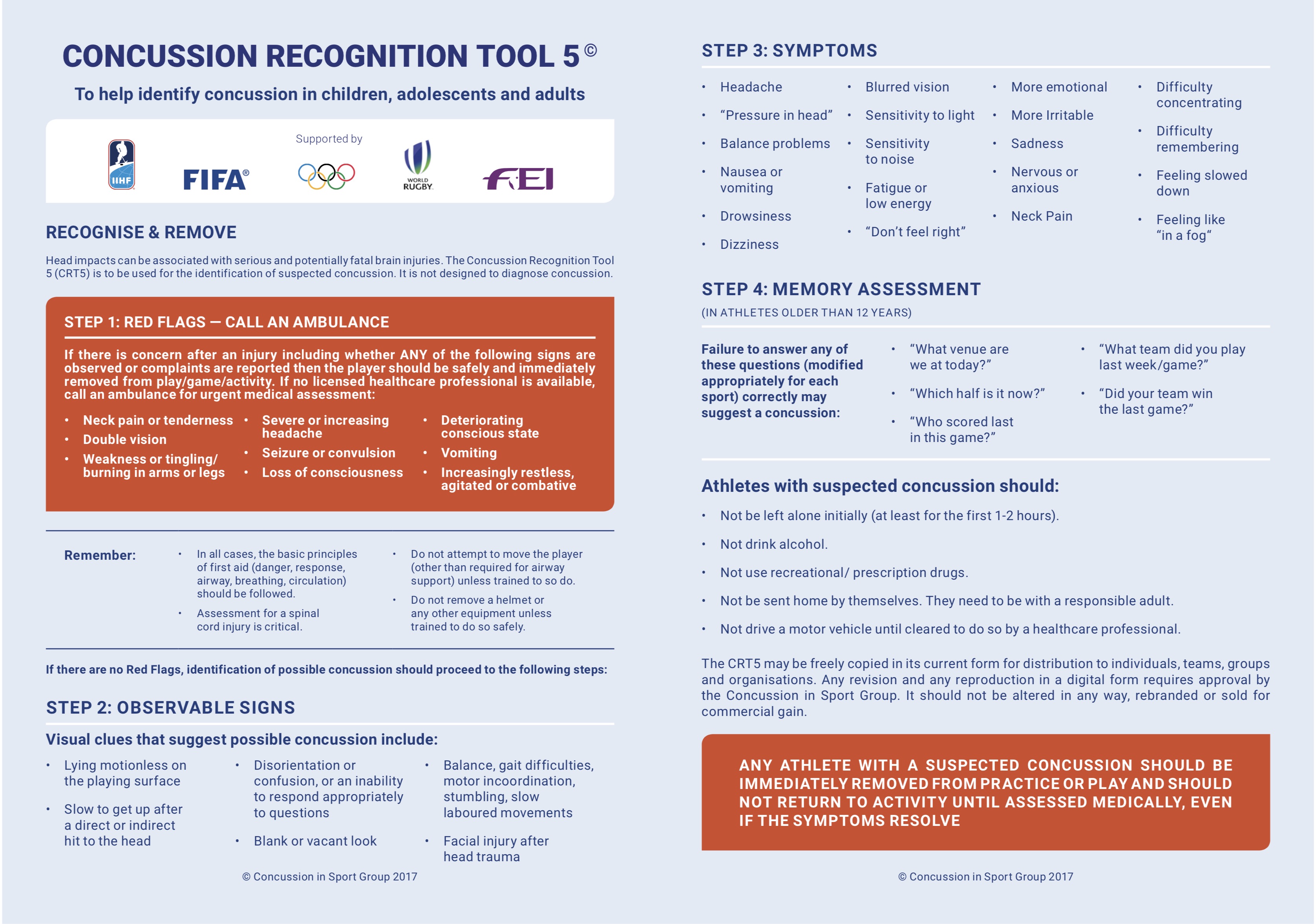
CRT5 – Concussion Recognition Tool
As a first aider you cannot diagnose concussion however it is also worthwhile to be familiar with the SCAT5 and child SCAT5, concussion assessment tools which are designed for use by medical practitioners to diagnose concussion.
First aiders should use CRT5 to help identify concussion in children, adolescents and adults.
Downloads
CRT5 Concussion Recognition Tool version 5, April 2017
SCAT5 Sport Concussion Assessment Tool version 5, April 2017
Child SCAT5 Sport Concussion Assessment Tool for children ages 5 - 12 years version 5, April 20
Consensus Statement on Concussion in Sport - 5th International Conference, Berlin 2016
Return to First Aid Tips List
Share this Tip
Related Courses
More Tips
- Ski Safe - Top tips to stay safe and injury free when skiing
- The Twelve Safety Tips of Christmas
- Cardiac Arrest in Young People
- CIMSPA Endorsed CPD Points
- Why should I train in first aid?
- Mental Health First Aider Support App - MHFA England
- Why don't we call abdominal thrusts the Heimlich manoeuvre anymore?
- First Aid Course Standard Hygiene Procedures
- What is an Automated External Defibrillator (AED)?
- Join our Team - Become a First Aid Trainer


